
In my former line of work (helping to support local public health departments from the position of a cubicle in the Capitol complex in St. Paul), much hay was made out of a notion of bridging a “rural-metro divide” between the Twin Cities and its surrounding suburbs and the rest of Minnesota. Indeed, overall, the arc of demography in Minnesota in the past half-century has been away from Greater Minnesota and toward the seven-county metro, including the Twin Cities and the surrounding areas.
It could be said that this sort of framing constitutes a “mental model” of geography and development in Minnesota — a set of “deeply held beliefs and assumptions and taken-for-granted ways of operating that influence how we think, what we do and how we talk,” as defined by John Kania and colleagues in their 2018 report on systems change. However, once I began living in the economically and culturally diverse Midway neighborhood of St. Paul, this model struck me as somewhat inaccurate.
Walking around, I saw many issues similar to ones raised in rural areas:
| Topic | Midway example | Rural example |
| Loss of retail | University Avenue retail, Midway Shopping Center | Retail stores, grocery stores |
| School closure | Richards Gordon Elementary (1911-1974) | Link |
| Hospital closure | Midway Hospital (~1927-1997) | Link |
| Old housing stock in need of rehabilitation | “[By 2037], the housing stock in most Saint Paul neighborhoods will be more than 100 years old” | Link |
Jokes aside about how much nicer the Roseville Target is relative to the one in the Midway, while just a few miles apart, such sights have made me question whether the binary between the “metro” and “Greater Minnesota” was entirely accurate.
Indeed:
- Greenhouse gas footprints in Minnesota are highest in suburban areas, not urban or rural ones.
- Visually, a ring of lower poverty rates in the metro suburbs exists between higher rates of poverty in rural Minnesota and inner Minneapolis-St. Paul.
- A less-pronounced, but still discernible sense of lower life expectancies in both very rural and very urban areas.
I have taken to refer to these visuals, where certain indicators for the metro suburbs stand in contrast to both Greater Minnesota and the cities of Minneapolis and St. Paul, as “donut theory,” or the notion that the true geographic divide in Minnesota is not between “Greater Minnesota” and the “metro,” but rather between the metro suburbs and everyone else.
For further, quasi-quasi scientific study of “donut theory,” I now turn my attention to the siting of hospitals in and around St. Paul.
Why Hospitals?
I selected hospitals as the focus of study because they are a salient example of public infrastructure, whose whole purpose is to serve people — and therefore, the location of hospitals ought to follow the location of people. Rural hospital closures are also known as an established issue, making it more practicable to draw comparisons between urban and rural issues on a common topic.
As the sole researcher on this study, my capacity constraints limited me to studying the fairer of the Twin Cities. Extensions of the analysis below to Minneapolis, as well as to the historic siting of public schools in both cities, are potential avenues for further study.
To the best of my abilities, I sought to locate every hospital within St. Paul’s city limits that was operational during a few select dates:
| Date | Reason for inclusion | Hospitals operational within city limits |
| 1960 | The peak of the city’s population (pop. 313,411) | 12 |
| 1980 | The “trough” of the city’s population loss (pop. 270,230) | 7, plus 2 children’s hospitals attached to a larger facility |
| 2020 | Peak contemporary population recovery, post-1960 (pop. 311,527) | 4, plus 2 children’s hospitals attached to a larger facility |
| 2025 | The present day (pop. ~307,465) | 3, plus 2 children’s hospitals attached to a larger facility, plus 1 behavioural health facility under construction |
A map of identified hospitals, with sources, is below:
A table of all hospitals included in the study is also as follows:
| Name | Location | Years active | Fate |
| Ancker | West Seventh | 1874-1965 | Replaced by St. Paul Ramsey (now Regions) Hospital |
| Bethesda | Frogtown | 1883/1932-present | Moved to former site of St. Joseph’s |
| Charles T. Miller | Downtown | 1920-1972 | Merged to become part of United Hospital |
| Children’s | West Seventh | 1928-present | Operational at United Hospital site |
| Divine Redeemer | South Saint Paul | 1960-1994 | Converted to a nursing home; demolished 2016 |
| Gillette Children’s | Payne-Phalen | 1908-present | Relocated to site at Regions Hospital in 1977 |
| Midway | Union Park | ~1927-1997 | Closed |
| Mounds Park | Dayton’s Bluff | 1906- ~1970s? | Converted into a senior living center |
| Regions | Downtown | 1965-present | Operational |
| Riverview Memorial | West Side | 1905-1980 | Merged to become part of United Hospital |
| Samaritan | Hamline Midway | ~1922-1987 | Closed |
| St. John’s | Dayton’s Bluff/Maplewood | 1915-present | Operational; relocated to Maplewood in 1987 |
| St. Joseph’s | Downtown | 1853-2020 | Closed |
| St. Luke’s | West Seventh | 1882-1972 | Merged to become part of United Hospital |
| TBD Behavioural Health hospital | Frogtown | TBD | Under construction |
| United | West Seventh | 1972-present | Operational |
| Woodwinds | Woodbury | 2000-present | Operational |
I welcome any corrections to the map and/or the tables. Send your corrections and ideas to [email protected].
Results and Discussion
A few trends immediately presented themselves:
- The consolidation of a larger number of dispersed facilities in town, to a smaller number of larger medical facilities in downtown.
- Relocation of hospitals to the suburbs.
- Loss of hospitals in many St. Paul neighborhoods, including the Midway, West Side and East St. Paul generally.
In the context of “donut theory,” this mapping exercise shows that St. Paul, too, has suffered from the loss of infrastructure (hospitals) within its boundaries, not unlike rural areas. For both, the driver for these closures is population decline, given that the demographics of Minnesota have shifted to the suburbs since the 1950s.
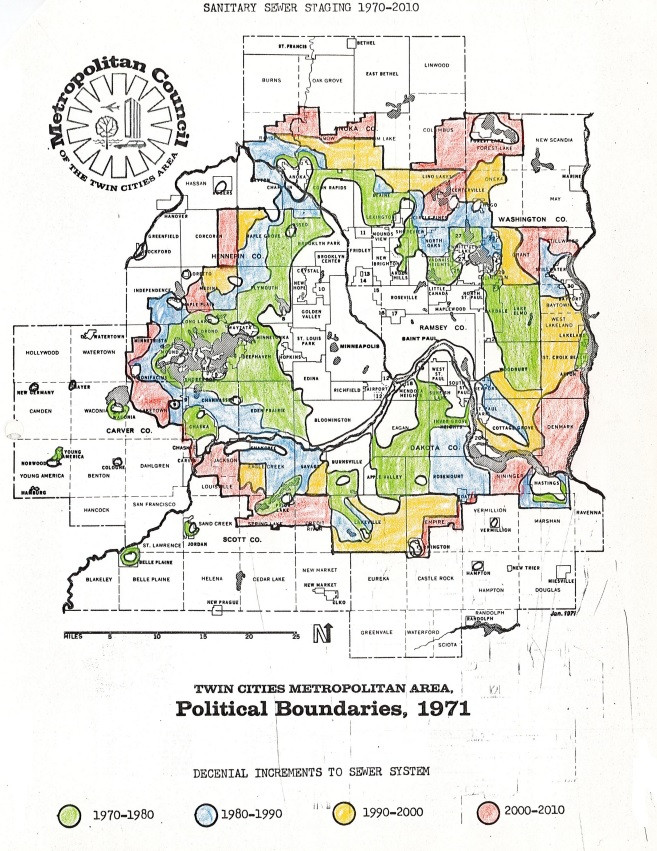
Below is a map showing the growth of the “donut” over the years. Courtesy of Todd Graham on Bluesky (@metrogram.bsky.social)
Although the changes in hospital location are, in large part, due to changing medical technology, patient needs and cost considerations, rather than an anti-urbanist conspiracy, the net result of these closures is to make it more difficult for people to reach medical facilities by foot, bicycle or transit. Interestingly, a study from 1974, commissioned by the Minnesota Department of Transportation’s (MnDOT) predecessor, the Department of Highways, found that the conversion of Highway 12 to I-94 in east St. Paul would have “the net effect of reducing accessibility to [Mounds Park Hospital].” Although an alternative solution was found to the point at issue (the loss of a nearby on-ramp), Mounds Park Hospital was closed later that decade, in spite of the study commenting that the hospital “could play a yet greater role in the delivery of healthcare in the future.”
In aggregate, the loss of urban facilities in St. Paul like Midway Hospital has also meant the loss of jobs to the suburbs, from custodians to surgeons.
On the public transit blog S(ubstack)-Bahn, author S.Y. Lee identified a “crisis of mobility” on multiple fronts in the United States:
Americans are getting squeezed on mobility, on all fronts
Americans are sleepwalking into a crisis of mobility — as a practice and as a right, both for self-interest and national health. Consider the following statistics:
S.Y. Lee End of the line: Transit thoughts in an uncertain America
- Most of the largest U.S. public transit agencies face a fiscal cliff, as aforementioned
- U.S. pedestrian fatality rates in 2023 by drivers were the highest since 1981
- U.S. car crash fatality rates (per 100k population) in 2023 rose back to 2007-levels after decade-long decline in the 2010s
- Americans spent nearly $50,000 on a new car in December 2024, the second highest month on record
- More than 80% of new car sales in the U.S. are trucks or SUVs, which are getting bigger and thus more likely to kill pedestrians or other drivers in crashes
- Car repair and maintenance costs have risen by nearly 40% since 2020
- Delinquencies on U.S. auto loans in 2024 hit highest levels since 2010
- National gas prices have stayed above $3 per gallon since 2021, the longest stretch since 2011-2014. (It is much higher in select regions, such as the West Coast.)
- All fifteen cities which recorded the largest population adds between 2022-2023 are in the South, per the U.S. Census. The top three cities — San Antonio, Fort Worth, and Charlotte — recorded, in sum, a daily ridership of ~145,000 in 2024. (Their total population: 3.5 million)
- Licensed drivers over the age of 65 has grown from 27.6 million in 2001 to 49.6 million in 2021, per NHTSA. Traffic deaths in 2022 involving drivers over the age of 65 was the highest since 1975.
The ability to access healthcare is essential for a fully realized life. But, within this contemporary crisis of American mobility, the trend of hospitals moving away from the urban core means that it is more difficult today for people to access medical facilities without a car, a public health risk in its own right.
Why Does Any of This Matter?
I explore “donut theory” vis-à-vis the extent to which mental models — which do not align with material reality as it exists — can cloud one’s judgement. At their worst, inaccurate mental models within the minds of policymakers can create poor public policy that fails to address its intended purpose, or even further worsen quality of life in society.
In urbanism, the prototypical inaccurate mental model, with disastrous consequences, is to view the city as a machine to be rationalized and planned meticulously, as in Le Courbusier’s concept for “La Ville radieuse” (The Radiant City) rather than as a vibrant ecosystem of people and place, as described by Jane Jacobs in “The Death and Life of Great American Cities.” The consequences of such mechanical thinking were the (mostly) failed schemes of urban renewal and slum clearance — in St. Paul, resulting in the construction of I-94 through the middle of the city, the demolition of neighborhoods such as Rondo and the sterile streetscape of downtown; in Minneapolis, much the same happened in the construction of urban highways, the demolition of neighborhoods like the Gateway District and vast, yet eerily quiet streetscapes in the center of the city.
The challenges Minnesota faces, now and tomorrow, are vast. Inequality is slowly but surely rising. In St. Paul, in particular, municipal finances are in disarray — a consequence of decades of stagnant population growth.
(Note: As an aside, for this reason I am sympathetic to Ward 4 City Council candidate Molly Coleman’s ideas for spurring development in St. Paul to increase the local tax base, including through upzoning, pre-approved plans and state action to legalize a land value tax, which all could incentivize and reduce regulatory barriers to expanded development in St. Paul.)
Climate change continues to be an increasingly salient issue, both in its impacts to land and people, as well as to the role that Minnesota plays in advancing or arresting the pace of climate change. The land of Minnesota also exists, like all of the other pieces of our country, subordinate to a federal government to whom the people of Minnesota pay taxes, and in return now receive harm and hostility.
At each of these junctures, the patterns of development and land use for nearly 80 years — suburban growth in exchange for both urban and rural stagnation or decline — exists as a culprit in these challenges:
- In relocating wealth and population away from the Twin Cities and rural areas alike.
- In the higher carbon footprint of suburban living.
- In the financial costs of sprawl, and the loss of farmland from sprawl, rather than investment in areas already developed.
Crucially, even with recent growth in housing and population, both Minneapolis and St. Paul have yet to recover their peak populations from 1950 and 1960, respectively.
It stands to reason as well that addressing any of these challenges will also entail policies and actions to redress the distribution of resources in Minnesota from out of the suburban “donut,” and back into the Twin Cities and rural areas alike.
It is my intention, and hope, that a carefully considered notion of “donut theory” better identifies sources and implications of geographic division and inequality in Minnesota, rather than the binary “Greater Minnesota/metro” dichotomy alone.